Communicating subclinical hypothyroidism with a patient
Subclinical hypothyroidism: Understand it before you explain it
Subclinical hypothyroidism is defined as:
TSH above reference range
Free T4 within normal range
TSH 4–10 mU/L → mild / borderline subclinical hypothyroidism
TSH >10 mU/L → higher risk of progression to overt hypothyroidism
How does a patient get a raised TSH but a normal T4? Let's look at the Hypothalamus-Pituitary-Thyroid axis
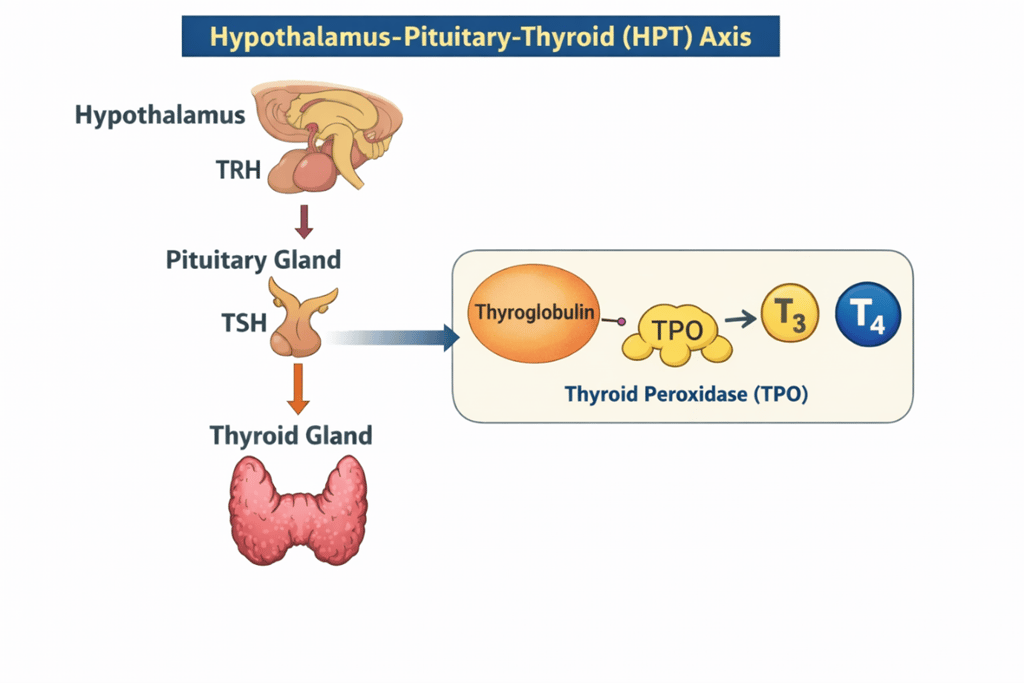
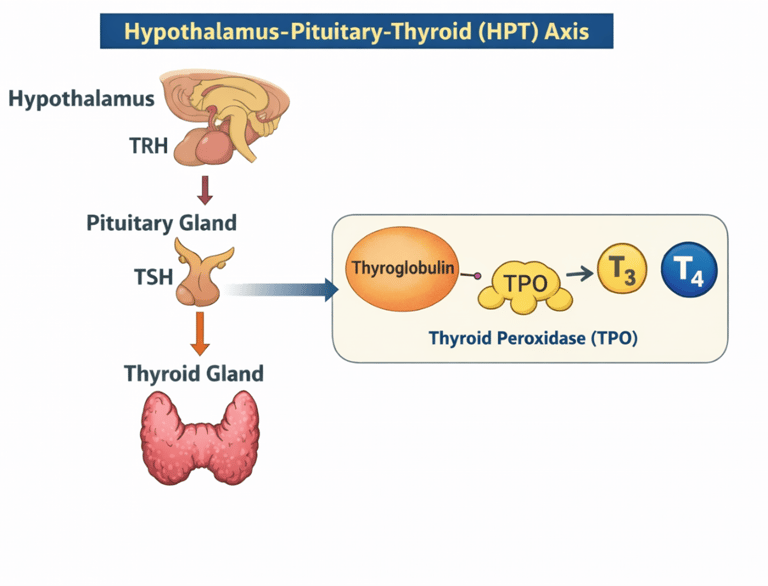
The hypothalamus produces Thyroid Releasing Hormone (TRH).
This activates the pituitary to produce Thyroid Stimulating Hormone (TSH).
This then acts on the thyroid gland to make T3 and T4. This process is done by Thyroid PerOxidase (TPO).
What does TPO do?
TPO causes conversion of thyroglobulin into T3 and T4 in the thyroid gland.
What is happening in the thyroid in subclincal hypothyroidism?
The hypothalamus and pituitary are producing enough TRH and TSH but the thyroid gland is struggling to make lots of T3/T4
Why do TSH levels rise?
The thyroid gland is slowing down, the hypothalamus and pituitary are producing more TRH and TSH to push the thyroid to work harder. Patients may have no symptoms, or mild non-specific symptoms.
What is Hashimotos Thyroditis?
This an autoimmune condition where the body produces TPO antibodies which attack TPO. TPO is needed for conversion of thyroglobulin to production of T3/T4.
If TPO is being attacked it can’t work as well so production of T3/T4 is compromised and levels of T3/T4 start to fall.
Are all cases of subclinical hypothyroidism due to early Hashimoto’s Disease?
No. Hashimoto’s thyroiditis is the most common cause, but not the only cause.
Roughly:
~60–80% → autoimmune (usually Hashimoto’s) – Positive TPO Antibody
~20–40% → non-autoimmune or transient causes
That uncertainty is exactly why we check TPO antibodies and look at trends, not just one TSH.
Causes of subclinical hypothyroidism
1. Autoimmune / Hashimoto’s thyroiditis (most common)
TPO antibodies often positive - the antibodies to TPO mean that the TPO is being 'attacked' by antibodies so less T3/T4 is being made
Higher risk of progression to overt hypothyroidism
2. Transient / reversible causes
These often resolve without treatment:
Recovery phase after non-thyroidal illness
Post-partum thyroiditis
TSH can lag behind T4 recovery thus giving a false impression of thyroid failure.
3. Physiological variation
Ageing (mild TSH rises can be normal)
4. Lifestyle & HPT-axis stress
Not autoimmune thyroid damage, but axis dysregulation:
Chronic psychological stress
Poor sleep
Under-nutrition / calorie restriction
Over-exercise
The thyroid gland may be structurally normal
5. Medications & iatrogenic causes
Lithium
Amiodarone
How does TPO status help you clinically?
TPO positive
Suggests autoimmune process
Higher likelihood of progression
Explains why the thyroid is struggling
Supports closer monitoring ± treatment later
TPO negative
Makes Hashimoto’s less likely (not impossible)
Raises possibility of:
Transient dysfunction
Lifestyle / stress factors
Physiological variation
Often stable or resolves
TPO antibodies predict trajectory, not current severity.
When should I treat subclinical Hypothyroidism?
NICE does NOT recommend routine treatment for everyone. Treatment is selective, based on TSH level, symptoms, and risk factors.
1. Treat if TSH is persistently ≥10 mU/L – the pituitary is working very hard to push an inefficient thyroid gland to keep working!
This is the clearest NICE indication.
Even if symptoms are mild or absent
Higher risk of progression to overt hypothyroidism
2. Consider treatment if TSH is 4–10 mU/L and one or more apply
Has symptoms consistent with hypothyroidism
Is TPO antibody positive
Has rising TSH on repeat testing
Is planning pregnancy or pregnant
Has cardiovascular risk factors
This is a shared decision. If asymptomatic and stable monitor rather than treat.
3. Do NOT routinely treat if:
TSH <10 mU/L with no clear symptoms
TPO antibodies negative
Stable or improving levels
Older adults (especially >65–70) with mild TSH elevation
Discussing results with the patient
You are not going to get lots of extra marks discussing the HPT axis and TPO in detail. With the exam keep it simple.
As per the pre-diabetes information sheet the word 'borderline' or drawing a scale can be useful and save you time.
The point of the case will be discussing whether it needs treating and why.
For example in the case below the TSH was 7 mU/L but the T4 was in normal range. A TPO has not been performed yet.
Doctor:
“So, your thyroid hormone level itself is within the normal range, but it’s at the lower end. We describe this as a borderline underactive thyroid. Do you know what thyroid gland does in our body?”
Patient:
“No”
Doctor:
“The thyroid is a small gland in your neck. It releases thyroid hormone that help controls your body’s metabolism. When its low your body’s functioning slows down”
Patient:
“What does that mean for me?”
Doctor:
“So, this is what we can discuss today. This slight low level could either mean than your thyroid is progressively slowing down (there a blood test that help us asses this) or it could be temporary. Right now your levels are not very low. We could re check bloods in 3 months. If the level falls even further we can treat it then.
However, if you are already having symptoms of low thyroid - like feeling tired - then we can treat this from today.
I was hoping we could explore if you are having any issues related to the thyroid to decide if treatment earlier might help you”
Patient:
“Ok doctor”
Doctor:
“So low thyroid can slow your body down.
What are your energy levels like? --> Patient answers
How is your sleep? --> Patient answers
Tell me about your appetite?” --> Patient answers
If the patient is displaying symptoms of low thyroid then you can suggest medication. This can be an opportunity for shared decision making.
Doctor:
“From what you have mentioned you are feeling tired and have very low energy levels. This may well be due to the borderline low thyroid levels. How would you feel about starting a low dose of thyroid medication today?”
With regards to the exam, you may have a case where the TPO has or hasn't been done. You will have to tailor your approach depending on the information you have in front of you.